Throughout your pregnancy, your baby will move around in your uterus. And, as your due date approaches, your baby will start to move into position for birth. Their positioning as you go into labor can be more or less favorable for a vaginal birth, which will dictate fewer or more potential complications.
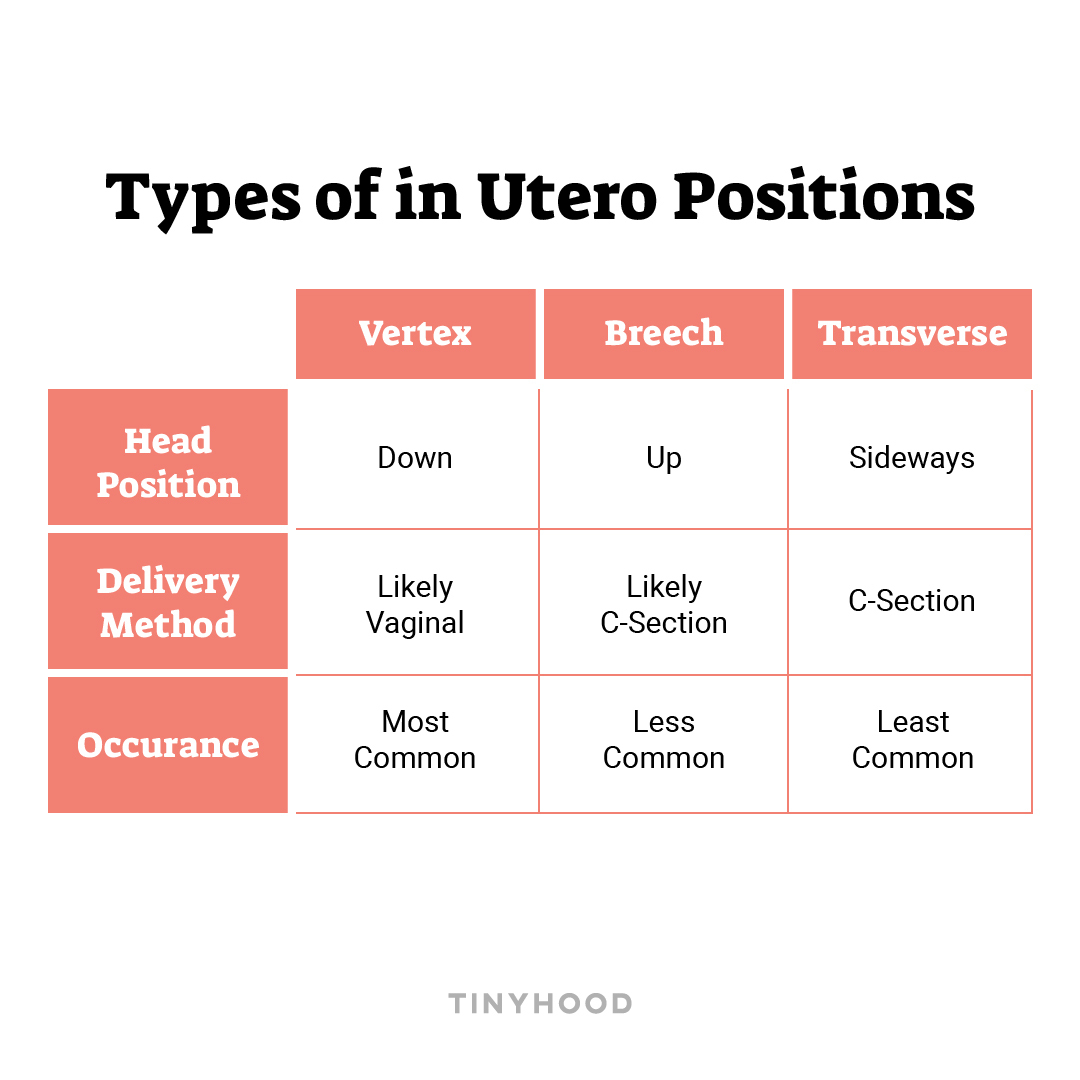
There are three possible positions that your baby can be in: Vertex, Breech, and Transverse — each with different variations. Ideally, when you go into the labor your baby will be in the Vertex position, meaning head down. If your baby ends up being in one of the two positions, your healthcare providers will take special considerations and action to either help move the baby into a more favorable position, or deliver the baby in another way. However, if you’re baby is in one of these less favorable positions, don’t panic — there are loads of ways to attempt to reposition them if needed.
Below, let’s take a closer look at each position, the variants within it, and the actions you and your healthcare provider could take depending on how your baby is positioned.
VERTEX
Vertex position is the most common position and is considered the optimal position because it allows the baby to flow through the movements that encourage a vaginal birth such as engaging into the pelvis, descending into the birth canal, and rotating through the pelvis and out of the vagina! This positioning also places pressure on the cervix and encourages dilation.
The most common position, when baby is head-down, happens in two ways:
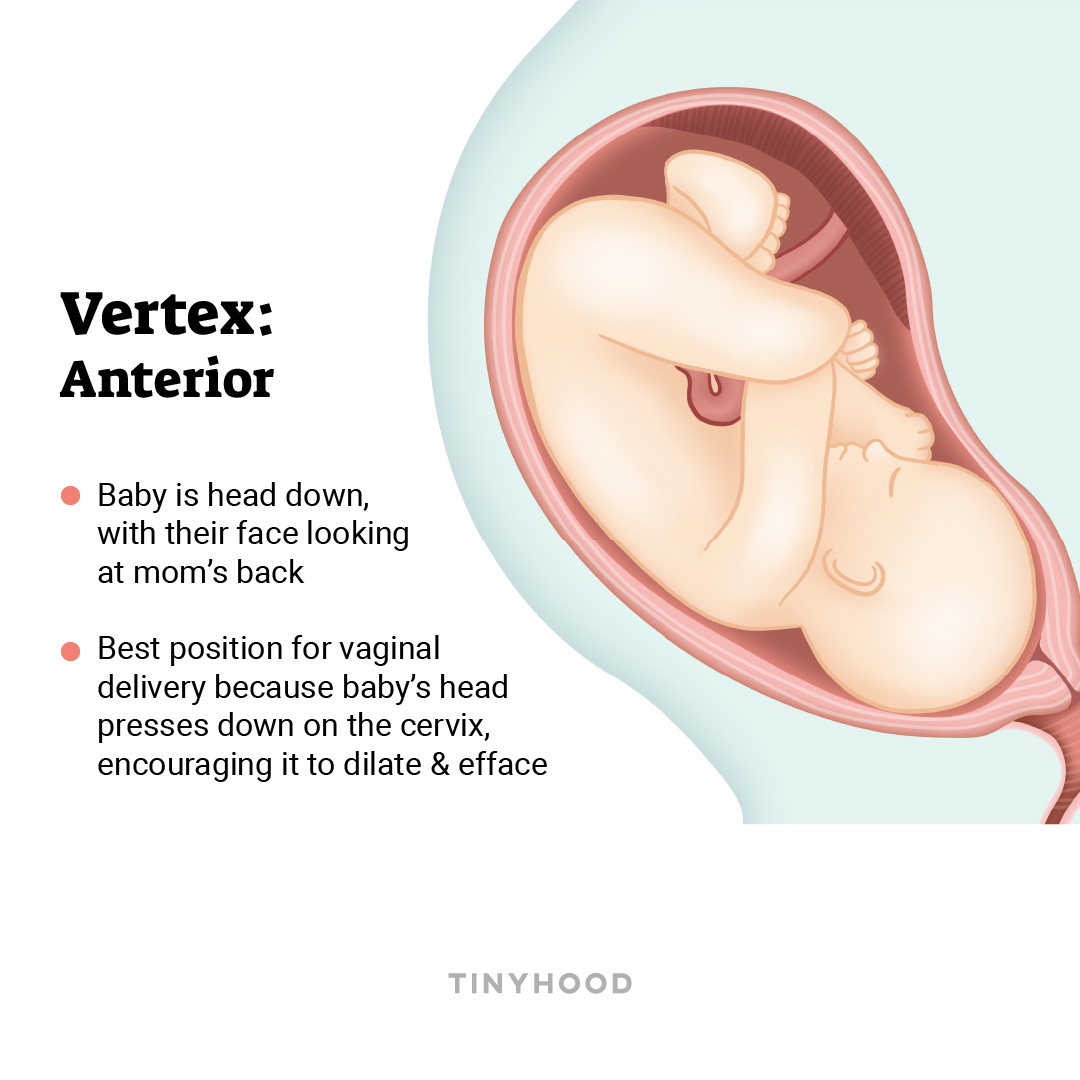
1. Occiput anterior
The most favorable birthing position, this is when the baby is head down, facing your back. Positioned this way, the baby’s head presses against the cervix, encouraging dilation and effacement.
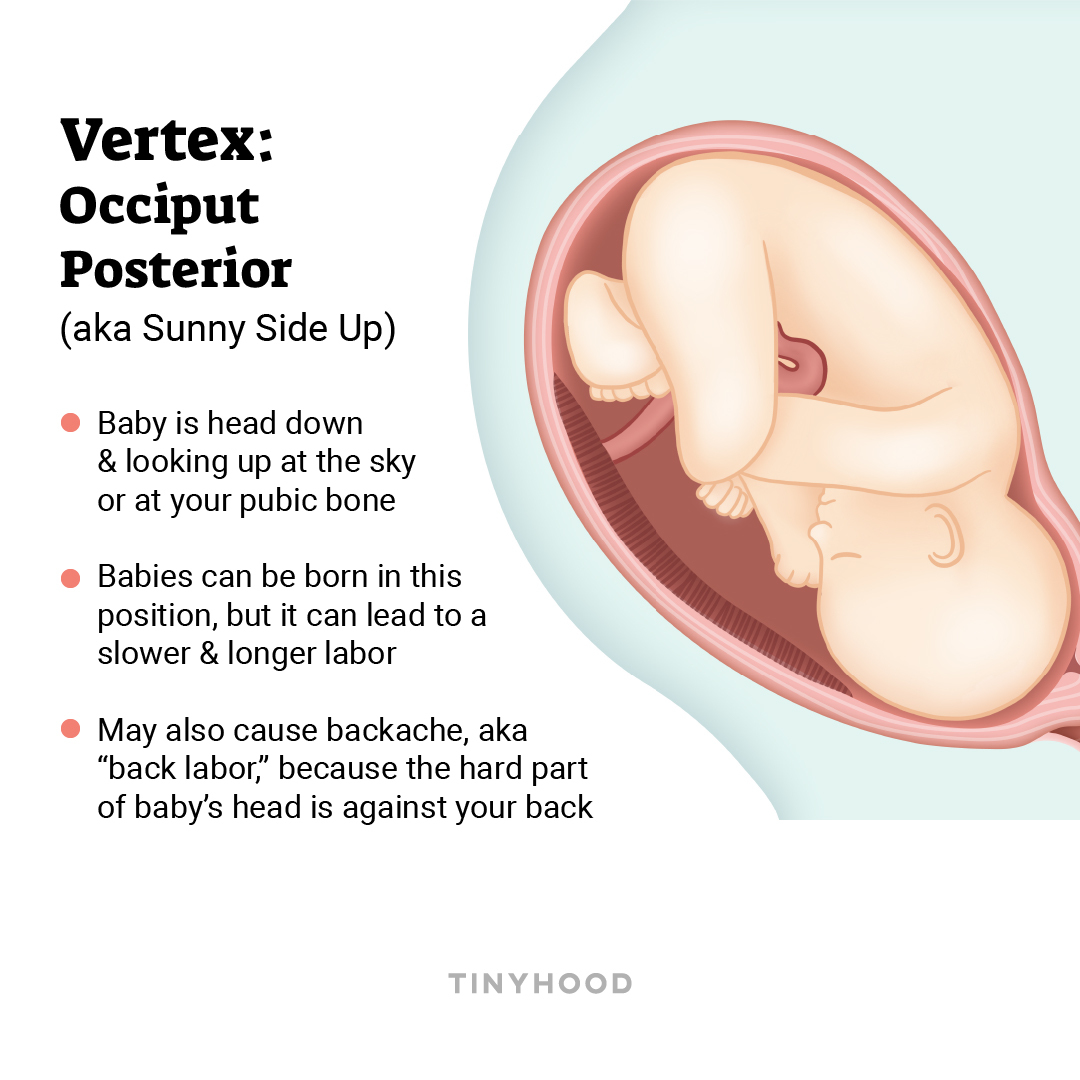
2. Occiput posterior
This is when the baby is head down, but looking forward, toward your pubic bone (also known as “sunny side up”).
Babies can be born this way, but labor might take longer, and you might experience more pain in your back (“back labor”) because the hard part of baby’s head is pressed against your back. Up to a third of babies start facing this way and spontaneously turn themselves as birth approaches. Only about 5-8% of babies are born in the occiput posterior position.
BREECH
Baby’s feet, buttocks, or knees are down toward the vagina, and the head is up by your ribs. Around 25% of babies are breech before 28 weeks, but only 3-4% are breech at term. Most providers do not perform breech vaginal deliveries because of concerns about the umbilical cord dangerously tangling around the baby, but you may be able to find a provider who will deliver vaginally if that is your preference.
There are three different breech positions:
1. Frank breech
Baby’s butt is down toward the bottom, with legs in front and feet close to the head.

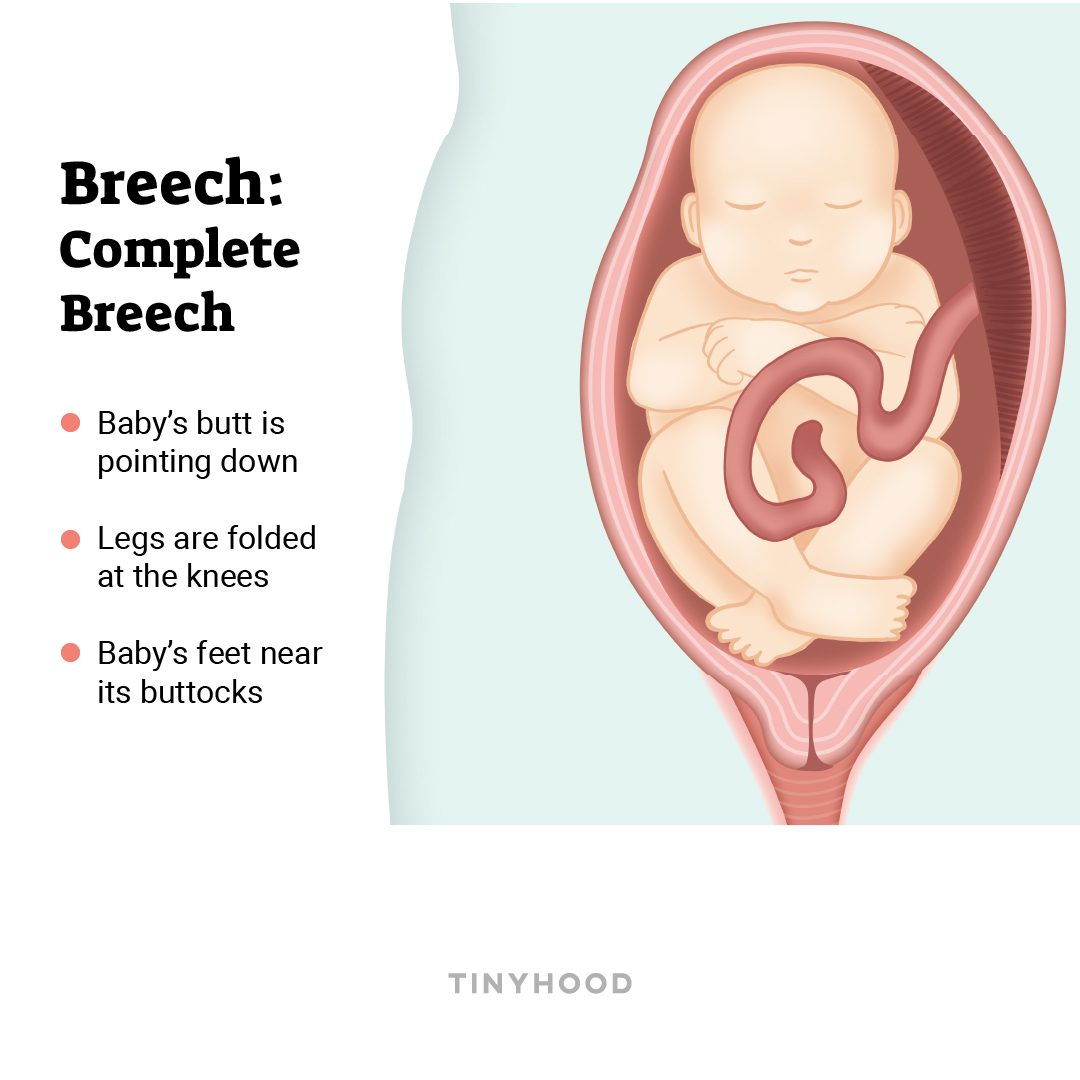
2. Complete breech
Legs are folded at the knees, with feet near baby’s buttocks.
3. Incomplete breech (footling)
One or both of baby’s feet are pointing down, leading the way.

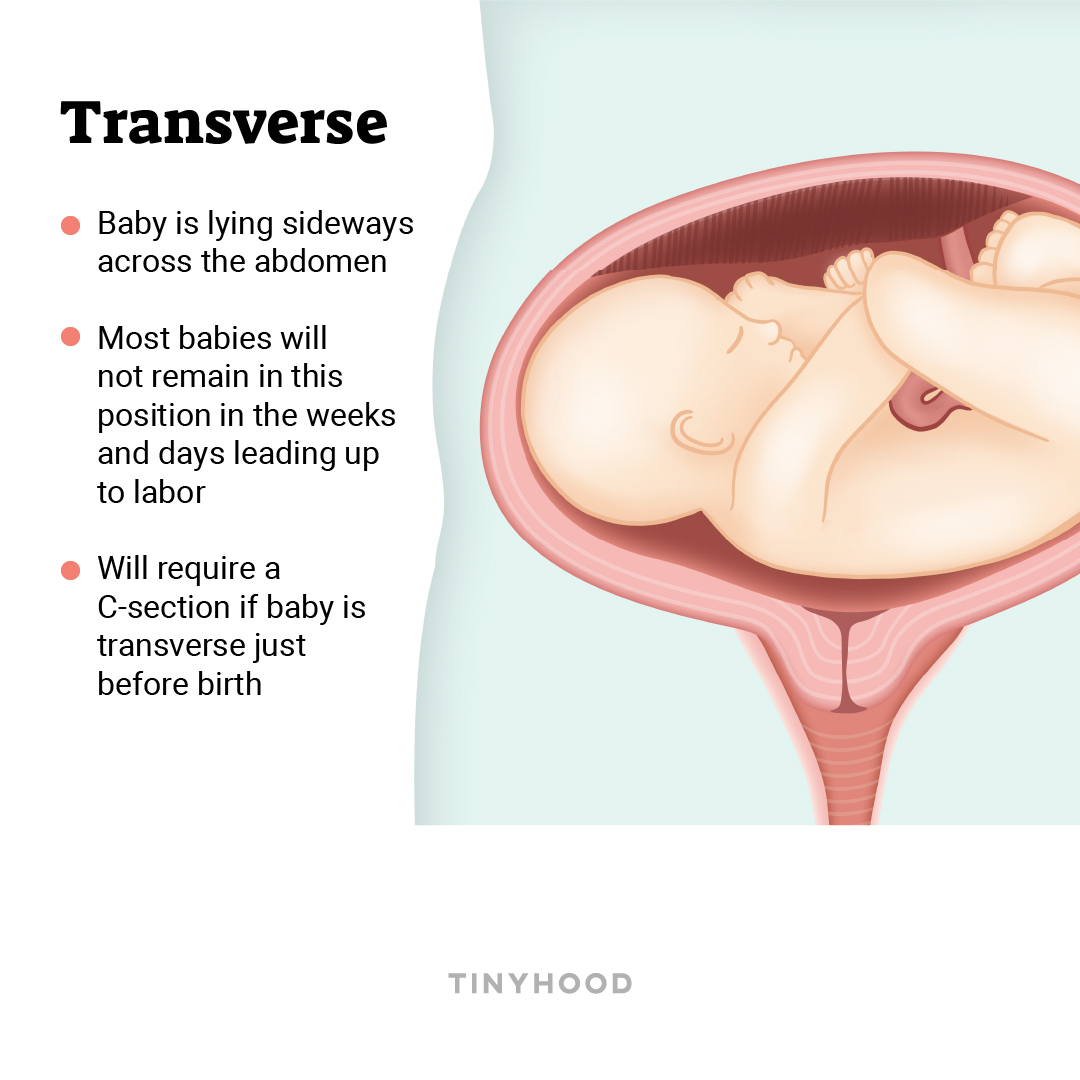
TRANSVERSE
Baby is lying sideways across your abdomen. Most babies will not remain in this position as labor nears, but a cesarean birth will be necessary if the baby does not move, as there is a risk of umbilical cord prolapse (delivering the cord before the baby).
REPOSITIONING
Your provider will begin assessing the baby’s position at 36-38 weeks, by using hands to feel your abdomen (called belly-mapping, or Leopold’s maneuver), or via ultrasound. After thirty-six weeks, it is unlikely the baby will change position on their own.
If baby is not vertex by thirty-six weeks, it is possible to try to reposition the baby to a more favorable position for vaginal birth. These options have a range of efficacy, and are to be attempted only with guidance from your provider.
External Cephalic Version (ECV, or a Version)
This is a procedure in which a provider uses the pressure of their hands on the outside of your abdomen to move the baby from a breech or transverse position to a vertex position. A provider will use an ultrasound for guidance, and tocolytic medicine to relax your uterus and prevent contractions. More than half of ECV’s are successful, but sometimes baby will move back into the breech or transverse position. Another ECV may be attempted, but the procedure is more difficult as pregnancy progresses and there is less room for movement in your uterus.
Gravity-based Strategies
It may be helpful to try to relax your pelvic muscles and use gravity to ease baby into position. Some ways to attempt this are through forward leaning inversion, lunges, squats, daily walks, and sitting on a chair backwards. There is not much scientific evidence that these methods work, but they are simple to attempt and there is no harm in trying them.
Chiropractic Adjustments
Some chiropractors are trained in a technique that uses gentle abdominal massage and small adjustments to the back to ease tension in the uterus (called the Webster technique). Be sure to consult your provider as there is little published research on this method.
Acupuncture and Moxibustion
Acupuncture is a method of inserting needles at different points of the body (acupoints) that are expected to influence the body. Moxibustion is a traditional Chinese method of burning herbs near the skin as a type of heat therapy and medicine. Some practitioners use acupuncture and moxibustion in combination to attempt to flip a breech baby. Speak with your provider if you are interested in these alternative methods.
Ice, Light and Sound
There are many ways to try to coax a baby down, and while there is no scientific evidence, some moms insist they work. You may try to create unpleasant sensations at the top of your abdomen, such as cold from an ice pack or bright light from a flashlight, to discourage baby from staying up high. Conversely, you could play pleasant music toward the bottom of your abdomen to encourage baby to move downward toward the sound.
For more information about baby positions, what they mean, and what you can do to change them, check out our course, Childbirth: What to Expect, Pain Management, and More and consult your healthcare provider.

About our Expert
Ashley Derderian Sousa is a board-certified lactation consultant and registered nurse with nearly ten years of experience in labor, delivery, and postpartum units. Through approachable methods and open and honest philosophy, she believes each journey to becoming a parent is a personal one that should be met with self-compassion. She is currently completing a Masters of Health Education.